The ear consists of three parts: the outer ear, the middle ear and the inner ear. Hearing loss can result from damage to any of these three parts. Hearing loss is a major public health issue and is the third most common physical condition after arthritis and heart disease.
Normal Ear Function
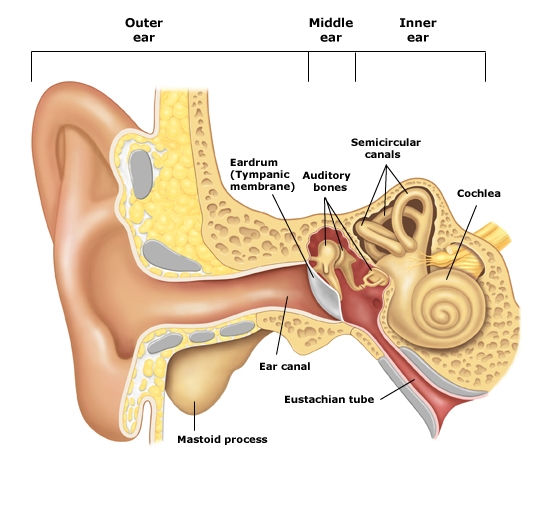
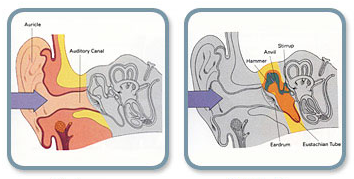
External Ear
Gathers sound waves and directs them towards the ear drum.
Middle ear
Transmits sound waves to the inner ear via vibration of Tympanic membrane (drum) and the three small ear bones: Malleus, incus and stapes.
Inner ear
Movement of the stapes stimulates the delicate hearing nerve endings which are bathed in Fluid In the inner ear(cochlea). Electric impulse is created and transmitted to the brain via hearing nerve , and is interpreted as sound.
Why do you need Hearing tests?
Hearing Tests determine the type and degree of hearing loss which will help the doctor to diagnose the pathology which causes Hearing loss.
1. Types of hearing loss
There are three types of hearing loss
2. Degree of Hearing loss
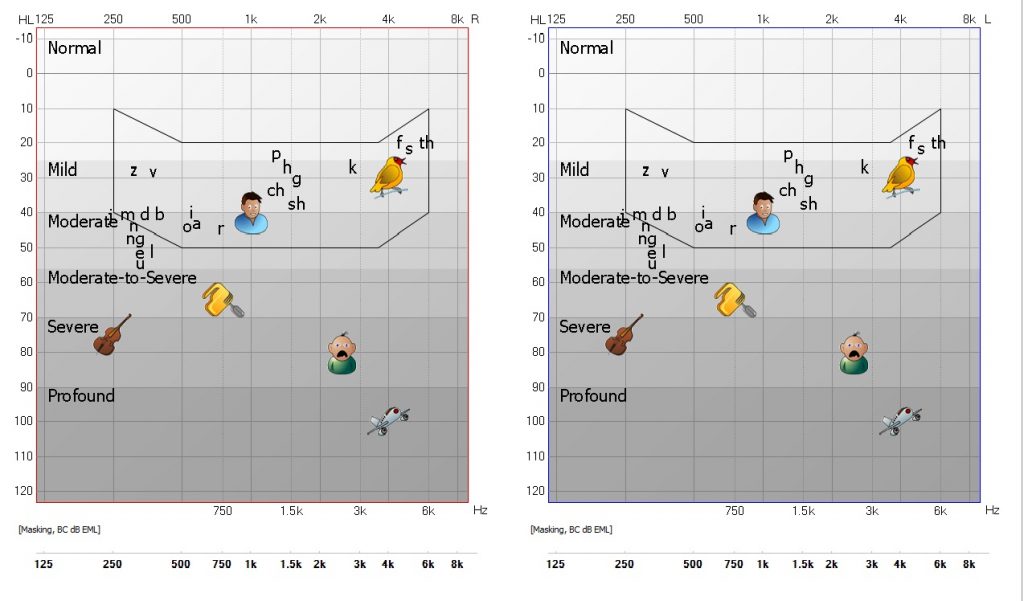
Normal Hearing: Hearing threshold between 10-20DBHL
Mild Hearing Loss: Hearing threshold between 25-40DBHL (8-15% hearing loss)
Patient will have difficulties in hearing soft or distant speech
Moderate Hearing loss: Hearing threshold between 40-65DBHL (20-45% hearing loss)
Patient will have trouble in hearing speech at normal conversation level
Severe Hearing loss: Hearing threshold between 65-90DBHL (60-90% hearing loss)
Patient will have difficulties in hearing loud speech
Profound Hearing Loss: Hearing threshold above 90 DBHL
Patient will not hear all environmental sounds
When do you need Hearing tests?
If you:
- Sometimes have difficulty understanding speech on the telephone or TV

- Find it difficult to follow a conversation in a noisy restaurant or crowded room
- Miss sometime a telephone ring or doorbell
- Hear ringing in your ears
- Expose so much to loud noises
If your baby:
- Doesn’t startle at loud noises
- Doesn’t turn to the source of a sound after 6 months of age
- Doesn’t say single words, such as “dada” or “mama” by 1 year of age
- Turns up the volume of the TV excessively high
- Respond inappropriately to questions

- Doesn’t reply when you call him/her
- Has articulation problems or speech/language delays
- Has difficulty understanding what people are saying
What are the hearing tests available in the clinic?
Adult Hearing tests
- Pure tone Audiometry

- Speech audiometry
- Free Field audiometry
- Assessment of Tinnitus
- High Frequency Audiometry
- Hearing aid counseling
- Tone decay test
- Acoustic reflexes decay test
Pediatric hearing tests
- Hearing screening for newborns

- Otoacoustic Emissions (TOAEs- DPOAEs)
- Auditory Brainstem Response (ABR)
- Conditioning Play Audiometry
- Visual Reinforcement Audiometry
- Multi-frequency Tympanometry
- Acoustic Reflexes testing
Otoacoustic Emissions OAE

Microphone is placed in the ear, sounds are played and a response is measured. If a baby hears normally, an echo is reflected back into the ear canal and is measured by the microphone (pass). When a baby has a hearing loss, no echo can be measured on the TOAE test (refer).
 Auditory Brainstem Response ABR
Auditory Brainstem Response ABR
Sounds are played to the baby’s ears. Electrodes are placed on the baby’s head to detect responses. This test measures how the hearing nerve responds to sounds and can identify babies who have hearing loss
Both tests work best when your baby is quiet and sleeping.
How is hearing loss treated or managed?
The treatment of choice may be medical, surgical, combination of these or Hearing aids.
The patients with conductive hearing impairment will never go deaf. They will always be able to hear, either with reconstructive ear surgery or by use of properly fitted hearing aid.
Most patients with sensoneural Hearing impairment may need hearing aids or cochlear implants decided according to the degree of hearing loss
 What are hearing aids?
What are hearing aids?
Hearing aids are sound-amplifying devices designed to aid people who have a hearing impairment.
Most hearing aids share several similar electronic components, including a microphone that picks up sound; amplifier circuitry that makes the sound louder; a miniature loudspeaker (receiver) that delivers the amplified sound into the ear canal; and batteries that power the electronic parts.
Hearing aids differ by:
- design
- technology used to achieve amplification (i.e., analog vs. digital)
- special features
What are cochlear Implants?
A cochlear implant is an electronic implantable medical device for people with severe-to-profound hearing loss. It works by transforming sounds into electrical signals and sending them to the auditory nerve. This means that it can bypass the damaged areas of the ear
Conductive Hearing loss
When the pathology lies in the external Ear or Middle Ear
A person with a conductive hearing impairment may notice that his ears seem to be full or plugged. He usually speaks softly, with a well-modulated voice, because he hears his own voice unduly loud. In general, Crunchy foods, such as celery, sound very loud and he may have stopped chewing to be able to hear what is being said. With this type of impairment one hears quite well over the telephone.
Fortunately, the patient with conductive hearing impairment will never go deaf. He will always be able to hear, either with reconstructive ear surgery or by use of properly fitted hearing aid.
Most common diseases causing conductive hearing loss
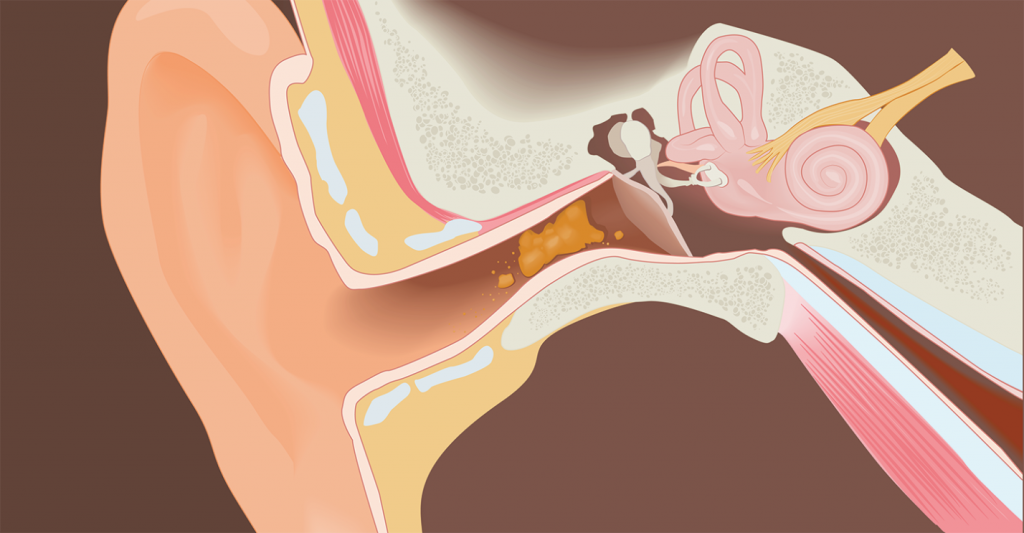
1. Impacted Wax or cerumen
Wax is sticky substance produced by glands located in the skin of the ear canal. It serves as an agent with protective, lubricating, and antibacterial properties. The absence of earwax may result in dry, itchy ears.
Most of the time, the old ear wax is moved out of our ear canal by the movement of jaws when chewing and by the movement of tiny hairs on the skin of the ear canal. Sometimes the self-cleaning process of the ears are affected and the wax instead of coming out, it is accumulated in the external ear canal (impacted Wax or Cerumen) thereby causing blockage and preventing the sound to transfer to the drum causing conductive hearing loss. In this case ear wax needed to be removed by suction or by special instrumentation under microscope (ear cleaning).
2. Otitis media with effusion
3. Perforation of tympanic membrane or eardrum
Tympanic membrane perforation is a hole or tears in the thin tissue that separates your ear canal from your middle ear (eardrum) and can result from disease (particularly infection) or trauma. Perforations can be temporary or persistent. Traumatic perforations occur from blows to the ear, severe atmospheric overpressure, exposure to excessive water pressure (scuba divers).
What are the symptoms of perforated eardrum?
Perforations without infection or cholesteatoma are not painful. The patient may complain from whistling sounds during sneezing and nose blowing, Conductive hearing loss, and a tendency to infection during colds and when water enters the ear canal. Perforation with infection results in purulent discharge.
How is tympanic membrane perforation diagnosed?
Most tympanic membrane perforations are diagnosed using routine otoscopy. Small perforations may require microscope for identification.
How is tympanic membrane perforation treated?
The goal of medical therapy for perforations is controlling ear discharge. Topically applied antibiotic eardrops may control the infection and ear discharge.
If the ear is dry for more than six months without any discharge, perforation can be treated by surgical procedure called Myringoplasty or tympanoplasty.
If there is cholesteotoma the patient needs surgical procedure called mastoidectomy
How to protect the ear with perforation in tympanic membrane
- Keep your ear dry. Place a waterproof silicone earplug or cotton ball coated with petroleum jelly in your ear when showering or bathing.
- Refrain from cleaning your ears by water.
- Avoid blowing your nose.
Myringoplasty
Myringoplasty is an operation carried out to repair a non-healing hole on your eardrum. It is done under general anaesthetic. A cut is made behind or above the ear. The material used to patch the eardrum is taken from under the skin. This eardrum ‘graft’ is placed against the eardrum. Dressings are placed in the ear canal. You may have an external dressing and a head bandage for a few days. The operation can successfully close a small hole nine times out of ten. The success rate is not quite so good if the hole is large.
4. Otosclerosis
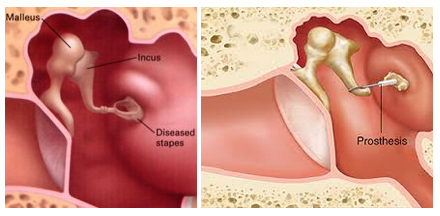
What is Otosclerosis?
Otosclerosis is a disease which affects the three small bones in the middle ear, more specifically the stapes. A part of the bone will grow abnormally and this bone growth will prevent the stapes from vibrating normally in response to sound.
What are the symptoms?
The patient will have gradual progressive hearing loss and buzzing sounds in both ears. The hearing loss will start in one of the ears and later it will bilateral.
What is the treatment of Otosclerosis?
In the early stages the hearing loss may only be minor and needs only observation. But if the hearing loss is progressed affecting on patient lifestyle, at some point something will need to be done.
There are two treatments available:
- 1- Hearing aids
- 2- Surgical treatment
Some patients like to try a hearing aid first and reserve surgery as a second option. However many patients do not like the thought of having to wear a hearing aid and therefore they go for surgery directly.
Stapedotomy
Stapedotomy is one of middle ear surgeries to restore hearing. It is for the patients suffering from Otosclerosis. It is done under general or local anaesthetic. The surgery is done through the ear canal; a small cut at the top of the ear canal may need to be made. The fixed part of stapes is removed and replaced by tiny piston. The vibrations from the eardrum can now be transmitted again to the inner ear. Restoring the patients hearing back.
Post-Operative Instructions: Tympanoplasty
Precautions:
- Do not blow your nose until your doctor has told you that your ear is healed. Any accumulated secretions in the nose may be drawn back into the throat and spit out if desired. The nose may be gently dabbed with tissue paper. This is particularly important if you catch a cold. You should follow this precaution for 4 weeks following surgery.
- Do not “pop” your ears by holding your nose and blowing air through the Eustachian tube into the ear.
- Sneeze with your mouth open.
- Do not allow water to enter your ear until advised by your doctor. The outer cap may be removed 48 hours after surgery. You may shower 48 hours after the operation. When showering, place a small clean piece of cotton dipped in Vaseline in your outer ear opening to keep water out. If you have packing in your ear, this may be placed directly over the packing. Remove the cotton after showering is complete.
- Avoid bending or heavy lifting (over 20 pounds) for three weeks following surgery.
- You may experience popping, clicking or other sounds in the ear. Your ear may also feel full. Occasional sharp shooting pains are not unusual. At times, it may feel as if there is liquid in your ear.
- Driving is permitted when you no longer experience dizziness or fatigue and you are no longer taking pain medication.
- Avoid flying for 3-4 weeks.
Sensoneural Hearing loss
When the Pathology lies in the inner Ear or in the neural pathways.
The person with this type hearing impairment may state that he can hear people talking but he cannot understand what they are saying(poor speech discrimination). An increase in the loudness of speech may only add to his confusion. Speech is audible but not clear to him. He usually hears better in quiet places and he may have difficulty understanding what is being said over the telephone. He will probably hear low tones better than high tones and, therefore, may find a man’s voice more understandable than a woman’s higher pitched voice. He may not hear a doorbell or the telephone ringing in another room.
Most common diseases causing sensorineural hearing loss
1. Presbycusis or age related hearing loss
Graduall loss of hearing in most people as they grow older. Age-related hearing loss most often occurs in both ears, affecting them equally.
There are many causes of age-related hearing loss. Most commonly, it arises from changes in the inner ear or in the nerve pathways from the ear to the brain as we age. Certain medical conditions and medications may also play a role.
2. Noise induced hearing loss
Loss of hearing because of exposure to loud sounds , The exposure may be one-time exposure but intense, such as an explosion or may be continuous exposure to loud sounds over long period of time, such as noise generated in a woodworking shop.
Some activities such as target shooting and hunting, snowmobile riding, listening to MP3 players at high volume through earbuds or headphones, playing in a band, and attending loud concerts can put you at risk for Noise induced hearing loss.
Can NIHL be prevented?
 NIHL is the only type of hearing loss that is completely preventable. Here’s how:
NIHL is the only type of hearing loss that is completely preventable. Here’s how:
- Know which noises can cause damage (those at or above 85 decibels).
- Wear earplugs or other protective devices when involved in a loud activity
- If you can’t reduce the noise or protect yourself from it, move away from it.
- Turn the volume down if you can
- Protect the ears of children who are too young to protect their own.

3. Meniere’s disease
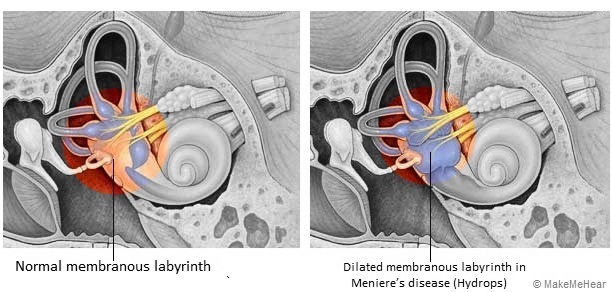
One of inner ear disorders which presents as recurrent attacks of spontaneous vertigo that last for minutes to hours accompanied by sensation of pressure or fullness in the ear and ringing in the ear. This can cause intermittent hearing loss only when having the attacks or gradual worsening of hearing or sudden hearing loss which is permanent.
An acute attack of Meniere’s disease is generally believed to result from increasing pressure of the fluid within the inner ear. This is called “hydrops”. One way for this to happen is when the drainage system, called the endolymphatic duct or sac is blocked or too much fluid secreted by the stria vascularis. In some cases, the endolymphatic duct may be obstructed by scar tissue, or may be narrow from birth.
It is diagnosed by hearing and balance tests
At the present time there is no cure for Meniere’s disease, but there are ways to manage the condition and to control the symptoms.
Self-Care and Home Treatment
- Diet and change of life style
Changing your diet may help to reduce the amount of fluid in the inner ear and ease symptoms. Items to limit or exclude from your diet include:
- salt
- caffeine
- chocolate
- alcohol
- monosodium glutamate (MSG)

It’s also important to drink six to eight glasses of water per day, so your body isn’t retaining fluid. Other lifestyle remedies include:
- resting during vertigo attacks
- eating regularly (to help regulate fluids in your body)
- managing anxiety and stress through psychotherapy or medication
It’s also important to quit smoking; nicotine can make the symptoms of Meniere’s disease worse.
Even though there’s no cure for Meniere’s disease, there are strategies you might want to consider to reduce your symptoms. Talk to your doctor about treatments that can help you cope with Meniere’s disease which may be.
- Medication
- Intratympanic injections
- Surgical treatment
Intratympanic Injections
Intratympanic injections can be used to treat Meniere’s disease. This means they are injected into the middle ear, through the ear drum. A procedure performed in the office.
This treatment is occasionally considered for patients with vertigo attacks not controlled by other medications and therapies
Procedure
The injections are performed with the patient lying down and using the office microscope. The ear is first cleaned of wax. A small area of the eardrum is numbed with a drop of medication. A small needle and syringe are then used and the needle is passed through the eardrum at the site that is numbed so that the tip is in the ear, near the round window. This is a membrane where drugs are absorbed in to the cochlea. The fluid is injected in to the middle ear and the patient stays lying down for 20-30 minutes during which he does not swallow or sniff. The drug sits against the round window and is absorbed in to the inner ear. The patient then sits up slowly and leaves the office. Patients should not drive for a few hours after this procedure. Water is kept out of the ear until it is confirmed that the tiny hole has healed.
In some patients, a ventilation tube is placed in to the eardrum and the medication is injected through the tube. This can allow the patient to self-treat with drops at home.
Complications
- A hole in the eardrum – This is a rare complication and it is higher when a ventilation tube is placed. The holes are usually small and can usually be repaired in the office.
- Dizziness – This is usually short lived.
- Loss of hearing – Depending on the particular therapies. In most cases are very rare.
- Infection – This is rare.
4. Acoustic Neuroma 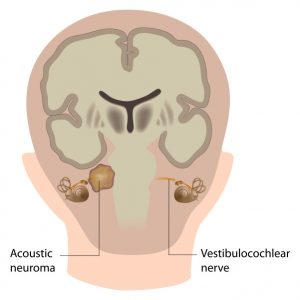
Benign slow growing mass that occasionally occurs on the hearing and balance nerve. It presents with hearing loss and tinnitus (sounds in the ear) in one side. Any patient with an unexplained progressive hearing loss and ringing sound only in one ear should get a MRI to rule out the tumor. Most commonly, an acoustic tumor is treated with surgery or radiation to prevent complications caused with ongoing tumor growth.
III-Mixed Hearing loss: When the pathology lies both in the middle & inner ear.
